Psycho-Oncology: Discover How Stress Causes Cancer
Phase 1 of Cancer: Inescapable Shock
Phase 2 of Cancer: Adrenaline Depletion
Phase 3 of Cancer: The Cancer Fungus
Phase 4 of Cancer: Niacin Deficiency
Phase 5 of Cancer: Vitamin C Depletion
Phase 6 of Cancer: Immune Suppression
PHASE 4 OF CANCER: NIACIN DEFICIENCY
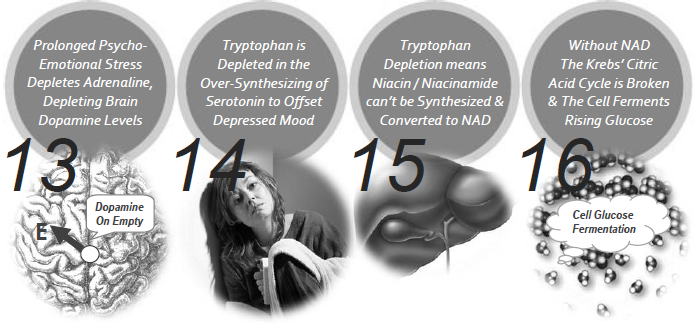
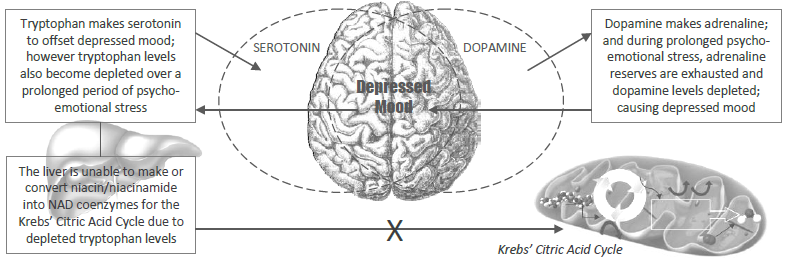
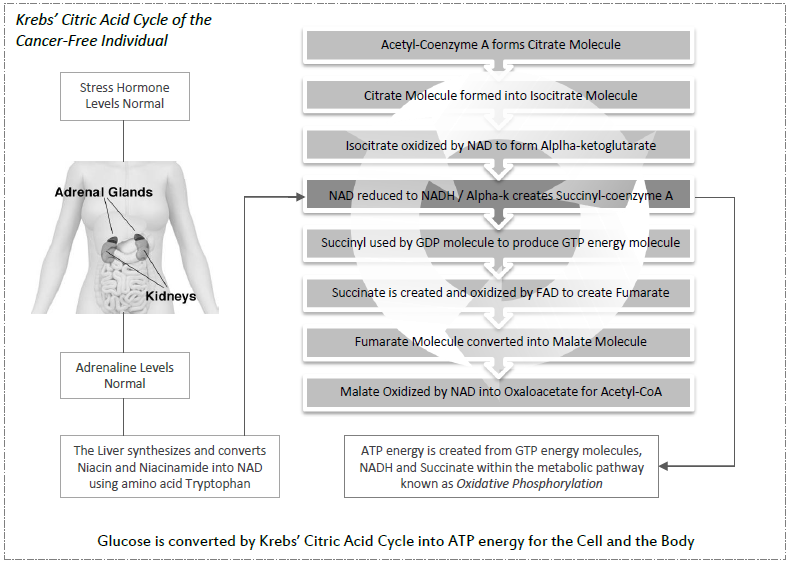
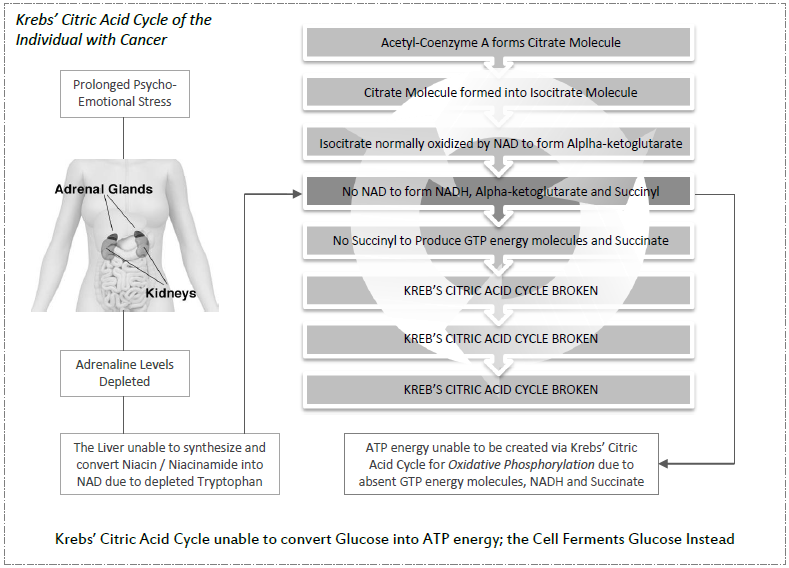
During phase 4, depleted adrenaline (epinephrine) levels cause a depletion of dopamine in the brain. Adrenaline is made by dopamine, and as more and more dopamine is used up during prolonged chronic stress, the amino-acid tryptophan creates serotonin to offset depressed mood. This results in a depletion of tryptophan which is needed to synthesize niacin / niacinamide (vitamin B3) for cell respiration. Normally tryptophan converts niacin / niacinamide into NAD coenzymes which are then used by the Krebs’ Citric Acid Cycle in the mitochondria of the cell for cell respiration, glucose conversion and the creation of ATP energy. Without niacin and NAD coenzymes, the Krebs' Citric Acid Cycle / Oxidative Phosphorylation metabolic pathway is broken, causing the cell to ferment glucose instead for energy, resulting in cell mutation and the formation of cancer.
THE THEORY: BY GLEN RUSSELL,
PUNA WAI ORA MIND-BODY CANCER CLINIC
In the 1950's, Dr Abram Hoffer, Director of Research at the Regina Psychiatric Services Branch, Dept. of Public Health, Canada, while administering high doses of oral vitamin C and niacin (vitamin B3) to patients hospitalized with psychiatric disorders, accidently found this combined treatment of vitamin C and niacin also effected a cure in a number of psychiatric patients with incurable cancer. Dr Hoffer subsequently went on to treat cancer patients in his own private practice from 1967 to 2005 and found the principle treatment of vitamin C and niacin in late stage cancer patients, whether undertaking chemotherapy, radiation or not, resulted in a life extension increase of 5.7 months [in the control group of 33 patients who did not follow his program] to 100 months on average [for the remaining 101 patients who did follow his program]. Dr Hoffer was particularly focused on the health properties of niacin—and for good reason—for niacin is crucial to the Krebs' Citric Acid Cycle, and in turn to the optimal functioning of the metabolic pathway Oxidative Phosphorylation. Niacin and niacinamide (also known as nicotinamide) are both forms of vitamin B3 and are synthesized [in the liver] from the amino acid tryptophan into coenzymes called NAD for the Krebs' Citric Acid Cycle to convert glucose into ATP energy for the cell and for the body. If this critical glucose-converting-ATP-energy-producing factory is shut down, then the cell is forced to ferment glucose instead via the process known as Glycolysis to obtain smaller amounts of ATP energy. This in turn creates a highly acidic low pH environment and the somatid [as mentioned in phase 3] pleomorphises within the body into viral-bacterial-yeast-like-fungus to ferment rising glucose levels in cells, causing normal cells to mutate into cancer cells. In cancer patients we see a chronic niacin deficiency caused by a chronic tryptophan deficiency. It takes 60mg of tryptophan for the liver to synthesize 1mg of niacin in the body, and when tryptophan is depleted so too is niacin. Tryptophan becomes depleted in the body when a person experiences prolonged psycho-emotional stress, as a result of stress depleting all-important adrenaline reserves. Adrenaline is made by dopamine, and as more and more dopamine is used up during stress, the amino-acid tryptophan synthesizes serotonin to offset depressed mood. This subsequently results in a depletion of serotonin and tryptophan, meaning niacin and niacinamide can no longer be created or converted by tryptophan into NAD coenzymes for the Krebs' Citric Acid Cycle for healthy cell functioning.
Dr Abram Hoffer [Clinical Procedures in Treating Terminally Ill Cancer Patients with Vitamin C + Niacin]: “I recall that in 1952 when I was working as a resident in psychiatry at the Munroe Wing which was a part of the General Hospital in Regina, a woman who had her breast removed for cancer was admitted to our ward. She was psychotic. This poor lady had developed a huge ulcerated lesion, she wasn’t healing, and she was in a toxic delirium. Her psychiatrist decided that he would give her shock treatment, which was the only treatment available at that time. I decided I would like to give her vitamin C instead. As director of research, I had the option of going to the physicians and asking them if I could do this with their patients. A friend of mine was her doctor and he said, “Yes, you can have her.” He said, “I’ll withhold shock treatment for three days.” I had thought that I would give her three grams per day, which was our usual dose at that time, for a period of weeks, but when he told me I could have three days only, I decided that this would not do. Therefore, I decided to give her one gram every hour. I instructed the nurses that she was to be given a gram per hour except when she was sleeping. When she awakened, she would get the vitamin C that she had missed. We started her on a Saturday morning and when her doctor came back on Monday morning to start shock treatment she was mentally normal. I wanted to know, if vitamin C would have any therapeutic effect. To our amazement her lesion on her breast began to heal. She was discharged, mentally well, still having cancer and she died six months later from her cancer. This was an interesting observation which I had made at that time and which I had never forgotten.
There was another root to this interest. In 1959, we found that the majority of schizophrenic patients excreted in their urine a factor that we call the mauve factor, which we have since identified as kryptopyrrole. I was looking for a good source of this urinary factor. We had thought that the majority of schizophrenics had it. We thought that normal people did not have it but I was interested in determining how many people who were stressed also had the factor. Therefore, I ran a study of patients from the University Hospital who were on the physical wards. They had all sorts of physical conditions including cancer, I found to my amazement that half the people with lung cancer also excreted the same factor. By 1960, a very famous gentleman of Saskatchewan, one of the professors retired and was admitted to the psychiatric department at our hospital. He was psychotic. He had been diagnosed as having a bronchiogenic carcinoma. It had been biopsied and was visualized in the x-ray and it had also been seen in the bronchoscope. While they were deciding what to do, he became psychotic so they concluded that he had secondaries in his brain. Because he became psychotic, he was no longer operable and instead they gave him cobalt radiation. It didn’t help the psychosis any. He was admitted to our ward where he stayed for about two months, completely psychotic. He was placed on the terminal list, I discovered that he was on our ward, so I thought he may have some mauve factor in his urine. On analysis he revealed huge quantities.
I had discovered by then that if we gave large amounts of B3 (Niacin) along with vitamin C to these patients, regardless of their diagnosis, they tended to do very well. He was started on three grams per day each of nicotinic acid (niacin) and ascorbic acid on a Friday. On Monday he was found to be normal. A few days later I said to him, "You understand that you have cancer?" He said, "Yes, I know that." He was friendly with me because I had treated his wife for alcoholism some time before. I said to him, "If you will agree to take these two vitamins as long as you live, I will provide them for you at no charge. In 1960, I was the only doctor in Canada that had access to large quantities of vitamin C and niacin. They were distributed through our hospital dispensary. He agreed. That meant he had to come to my office every month in order to pick up two bottles of vitamins. I didn't know that it might help his cancer. I was interested only in his psychological state. However, to my amazement he didn't die. After 12 months, I was having lunch with the director of the cancer clinic, a friend of mine, and I said to him, "What do you think about this man?" And he said, "We can't understand it, we can't see the tumor any more." I thought he'd say, "Well, isn't that great." So I asked, "Well, what's your reaction?" He responded, "We are beginning to think we made the wrong diagnosis." The patient died, 30 months after I first saw him, of a coronary. Here's another case that is very interesting. A couple of years later, a mother I had treated for depression came back to see me. Once more she was depressed. She said she had a daughter 16, who had just been diagnosed as having an osteogenic sarcoma of the arm. Her surgeon had recommended that the arm be amputated. She was very depressed over this and so I asked her, "Do you think you can persuade your surgeon not to amputate the arm right away?" And I told her the story about the man with the lung cancer. She brought her daughter in and I started her on niacinamide, 3 grams per day, plus vitamin C, three grams per day. She made a complete recovery and is still well, not having had to have surgery. But this time I concluded that maybe B-3 (niacin) was the therapeutic factor. The reason for that, of course, is very simple. I liked B3 and I didn't have much interest in vitamin C.
When I moved to Victoria, another strange event happened. In 1979, a woman developed jaundice and during surgery a six centimetre in diameter lump in the head of the pancreas was found. They were too frightened to do a biopsy, which apparently is quite standard. They thought that the biopsy might disseminate the tumor. The surgeon closed and told her to write her will. They said she might have three to six months at the most. She was a very tough lady and she had read Norman Cousins' book Anatomy of an Illness. So she said to her doctor, "To hell with that, I'm not going to die." And she began to take vitamin C on her own, 12 grams per day. When her doctor discovered what she was doing, he asked her to come and see me, because by that time I was identified as a doctor who liked to work with vitamins. I started her on 40 grams of vitamin C per day, to which I added niacin, zinc and a multivitamin, multi-mineral preparation. I had her change her diet by staying away from high protein and fat. I didn't hear from her again for about six months. One Sunday, she called me. Normally when I get a call from a patient on a Sunday, it's bad news. She immediately said, "Dr Hoffer, good news! I asked, "What's happened?" She said, "They have just done a CT scan and they can't see the tumor," So then she said, "They couldn't believe it. They thought the machine had gone wrong; so they did it all over again. And it was also negative the second time." She had her last CT scan in 1984, no mass, and she is still alive and well today.
There was another root to this interest. In 1959, we found that the majority of schizophrenic patients excreted in their urine a factor that we call the mauve factor, which we have since identified as kryptopyrrole. I was looking for a good source of this urinary factor. We had thought that the majority of schizophrenics had it. We thought that normal people did not have it but I was interested in determining how many people who were stressed also had the factor. Therefore, I ran a study of patients from the University Hospital who were on the physical wards. They had all sorts of physical conditions including cancer, I found to my amazement that half the people with lung cancer also excreted the same factor. By 1960, a very famous gentleman of Saskatchewan, one of the professors retired and was admitted to the psychiatric department at our hospital. He was psychotic. He had been diagnosed as having a bronchiogenic carcinoma. It had been biopsied and was visualized in the x-ray and it had also been seen in the bronchoscope. While they were deciding what to do, he became psychotic so they concluded that he had secondaries in his brain. Because he became psychotic, he was no longer operable and instead they gave him cobalt radiation. It didn’t help the psychosis any. He was admitted to our ward where he stayed for about two months, completely psychotic. He was placed on the terminal list, I discovered that he was on our ward, so I thought he may have some mauve factor in his urine. On analysis he revealed huge quantities.
I had discovered by then that if we gave large amounts of B3 (Niacin) along with vitamin C to these patients, regardless of their diagnosis, they tended to do very well. He was started on three grams per day each of nicotinic acid (niacin) and ascorbic acid on a Friday. On Monday he was found to be normal. A few days later I said to him, "You understand that you have cancer?" He said, "Yes, I know that." He was friendly with me because I had treated his wife for alcoholism some time before. I said to him, "If you will agree to take these two vitamins as long as you live, I will provide them for you at no charge. In 1960, I was the only doctor in Canada that had access to large quantities of vitamin C and niacin. They were distributed through our hospital dispensary. He agreed. That meant he had to come to my office every month in order to pick up two bottles of vitamins. I didn't know that it might help his cancer. I was interested only in his psychological state. However, to my amazement he didn't die. After 12 months, I was having lunch with the director of the cancer clinic, a friend of mine, and I said to him, "What do you think about this man?" And he said, "We can't understand it, we can't see the tumor any more." I thought he'd say, "Well, isn't that great." So I asked, "Well, what's your reaction?" He responded, "We are beginning to think we made the wrong diagnosis." The patient died, 30 months after I first saw him, of a coronary. Here's another case that is very interesting. A couple of years later, a mother I had treated for depression came back to see me. Once more she was depressed. She said she had a daughter 16, who had just been diagnosed as having an osteogenic sarcoma of the arm. Her surgeon had recommended that the arm be amputated. She was very depressed over this and so I asked her, "Do you think you can persuade your surgeon not to amputate the arm right away?" And I told her the story about the man with the lung cancer. She brought her daughter in and I started her on niacinamide, 3 grams per day, plus vitamin C, three grams per day. She made a complete recovery and is still well, not having had to have surgery. But this time I concluded that maybe B-3 (niacin) was the therapeutic factor. The reason for that, of course, is very simple. I liked B3 and I didn't have much interest in vitamin C.
When I moved to Victoria, another strange event happened. In 1979, a woman developed jaundice and during surgery a six centimetre in diameter lump in the head of the pancreas was found. They were too frightened to do a biopsy, which apparently is quite standard. They thought that the biopsy might disseminate the tumor. The surgeon closed and told her to write her will. They said she might have three to six months at the most. She was a very tough lady and she had read Norman Cousins' book Anatomy of an Illness. So she said to her doctor, "To hell with that, I'm not going to die." And she began to take vitamin C on her own, 12 grams per day. When her doctor discovered what she was doing, he asked her to come and see me, because by that time I was identified as a doctor who liked to work with vitamins. I started her on 40 grams of vitamin C per day, to which I added niacin, zinc and a multivitamin, multi-mineral preparation. I had her change her diet by staying away from high protein and fat. I didn't hear from her again for about six months. One Sunday, she called me. Normally when I get a call from a patient on a Sunday, it's bad news. She immediately said, "Dr Hoffer, good news! I asked, "What's happened?" She said, "They have just done a CT scan and they can't see the tumor," So then she said, "They couldn't believe it. They thought the machine had gone wrong; so they did it all over again. And it was also negative the second time." She had her last CT scan in 1984, no mass, and she is still alive and well today.
Abram Hoffer
The last case I'm going to give details of one born in 1908. His mother died of cancer and his father had a coronary at the age of 80. My patient had had a myocardial infarction in 1969, and again in 1977, followed by a coronary bypass. In March on 1978, he suddenly developed pain in his left groin and down the left leg. In February 1979, he developed a bulge in his left groin, and later, severe pain with movement. In surgery, a large mass infiltrating sarcoma was found, part of which was removed, but a mass the size of a grapefruit was left. The tumor was eroding into a ramus of the pubic bone. They concluded that it was not radio-sensitive. In March he had palliative radiation to his left half - 4500 rads. The pain was gone at the end of the radiation. On May 28, he developed a severe staph infection, and in June he was very depressed because his wife was dying of cancer and also he was suffering from drainage of chronic infection. In July he still had a purulent discharge in two areas. Now the mass was visible and palpable in the left iliac area above the inguinal ligaments. In January of 1980, he saw me for the first time. I started him on 12 grams of vitamin C per day and I recommended to his referring doctor that he give him IV ascorbic acid, 2.5 grams, twice per week, which he agreed to. I gave him niacin, vitamin B6 and zinc to balance it out. In April, the mass began to regress and the oncologist wrote, "This is interesting, it must be something else." In other words, the patient said, the vitamin C is helping and the oncologist said, no it isn't. The oncologist put a note in the file, "He's probably responding to chemotherapy." But he had never had chemotherapy. The infection was gone. In May 1980, his x-ray showed reconstruction of the left superior pubic ramus. In July he wrote to me telling how grateful he was to be so well. In February of 1988, he went back to the cancer clinic for some recurrent facial skin carcinoma. He died in the fall of 1989 of coronary disease when he was 81. This man survived 10 years after having been diagnosed with cancer.
I examined every cancer patient referred to me between July 1978 and April 1988 and followed them to January 1990. I did not miss a single case. A total of 134 were seen. And I dated the time that they first saw me as day zero. The only thing I wanted to look at was survival. I wanted hard data, something that couldn't be argued within. I wasn't going to say the patients were better or not better because these are subjective terms. These 134 fell into two groups. It wasn't my fault that this happened because I treated every one of them exactly the same way. I did not plan a double blind prospective study. What I planned and what I did was to advise every patient what I thought they ought to do in terms of their cancer. If they were getting radiation, I suggested they stay with it. If they were getting chemotherapy, I suggested they stay with that. I never advised them about their surgery, chemotherapy or radiation. However, out of these 134, there were 33 who did not or could not follow the program. For example, on chemotherapy, they were so nauseated that they couldn't hold anything down and if they couldn't hold the vitamins down they weren't going to do very much good. There were some who didn't believe in the program. [Note: Dr Hoffer and Linus Pauling revised this number in official literature to 132 patients and 31 not following the program.]
The other 101 did stay on their program at least two months. Some went off in the third or fourth month but they stayed on it for at least two months. I was encouraged by Linus Pauling. I followed them all. First of all, I contacted their doctors. I contacted the patients that were still alive. I contacted their families. I got all their records from the cancer clinics. I had a complete file on every patient I had seen so that I knew within a matter of months exactly what had happened to them. The results were analysed by Dr. Linus Pauling using a new technique for analyzing cohorts. The data is as follows: 33 [later 31] controls - they survived an average of 5.7 months, from the first day that I saw them. There were two treatment cohorts: a cohort of 40 females with cancer of the breast, ovary, uterus or cervix. The second cohort of 61 were other types of cancer. The cohorts were divided into two groups. First were the poor responders, those who didn't do well (20% of patients); they survived an average of 10 months, nearly twice as long as the control. The others, the good responders (80% of patients), were divided into two groups. The female group survived an average of 122 months and the other group 72 months. I think this is very significant. There was a tremendous difference in the survival rate. Today, all the controls are dead, 50% of the treated group are still alive. Over the past year, I did another survey and of the remainder only three more have died. It cannot be all due to cancer because I'm dealing with a population with ages between 60 and 80. They are going to die of other causes as well. This was published in the Journal of Orthomolecular Medicine, Volume 5, p. 143, 1990.
Within the 4th Phase of Cancer the following sequence of events can be observed in the cancer patient:
I examined every cancer patient referred to me between July 1978 and April 1988 and followed them to January 1990. I did not miss a single case. A total of 134 were seen. And I dated the time that they first saw me as day zero. The only thing I wanted to look at was survival. I wanted hard data, something that couldn't be argued within. I wasn't going to say the patients were better or not better because these are subjective terms. These 134 fell into two groups. It wasn't my fault that this happened because I treated every one of them exactly the same way. I did not plan a double blind prospective study. What I planned and what I did was to advise every patient what I thought they ought to do in terms of their cancer. If they were getting radiation, I suggested they stay with it. If they were getting chemotherapy, I suggested they stay with that. I never advised them about their surgery, chemotherapy or radiation. However, out of these 134, there were 33 who did not or could not follow the program. For example, on chemotherapy, they were so nauseated that they couldn't hold anything down and if they couldn't hold the vitamins down they weren't going to do very much good. There were some who didn't believe in the program. [Note: Dr Hoffer and Linus Pauling revised this number in official literature to 132 patients and 31 not following the program.]
The other 101 did stay on their program at least two months. Some went off in the third or fourth month but they stayed on it for at least two months. I was encouraged by Linus Pauling. I followed them all. First of all, I contacted their doctors. I contacted the patients that were still alive. I contacted their families. I got all their records from the cancer clinics. I had a complete file on every patient I had seen so that I knew within a matter of months exactly what had happened to them. The results were analysed by Dr. Linus Pauling using a new technique for analyzing cohorts. The data is as follows: 33 [later 31] controls - they survived an average of 5.7 months, from the first day that I saw them. There were two treatment cohorts: a cohort of 40 females with cancer of the breast, ovary, uterus or cervix. The second cohort of 61 were other types of cancer. The cohorts were divided into two groups. First were the poor responders, those who didn't do well (20% of patients); they survived an average of 10 months, nearly twice as long as the control. The others, the good responders (80% of patients), were divided into two groups. The female group survived an average of 122 months and the other group 72 months. I think this is very significant. There was a tremendous difference in the survival rate. Today, all the controls are dead, 50% of the treated group are still alive. Over the past year, I did another survey and of the remainder only three more have died. It cannot be all due to cancer because I'm dealing with a population with ages between 60 and 80. They are going to die of other causes as well. This was published in the Journal of Orthomolecular Medicine, Volume 5, p. 143, 1990.
Within the 4th Phase of Cancer the following sequence of events can be observed in the cancer patient: